General Features
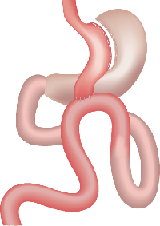
Just as in the case of a RNY Gastric Bypass operation, the stomach is divided into two parts.
The difference with RNY Gastric Bypass is that the small bowel is connected to the stomach without dividing the small bowel.
By doing like this, the procedure consists of a single anastomosis.
Bypassing a longer segment of the small bowel tract (than the RNY Gastric Bypass operation) causes more malabsorption.
The main disadvantage is that bile can directly enter the stomach (or even in the esophagus). Chronic bile reflux could be associated with an elevated risk of malignancy and is the reason Mini Gastric Bypass is still not officially approved in the USA.
Based on scientific research, weight loss in our patients occurs as follows.
| * AT 6 WEEKS: | From the initial weight | -%10 |
|---|---|---|
| * AT 3 MONTHS: | From the initial weight | -%15 |
| * AT 6 MONTHS: | From the initial weight | -%20 - 25 |
| * AT 9 MONTHS: | From the initial weight | -%25 - 30 |
| * AT 12 MONTHS: | From the initial weight | -%35 - 40 |
These numbers may vary depending on the eating, drinking and exercising habits of the patient..
RISKS AND COMPLICATIONS:
| Short term | Long term |
|---|---|
| Leakage | Anastomotic ulcer |
| Bleeding | Intestinal Obstruction |
| Respiratory Infection | Incisional hernia |
| Embolism | |
| Incisional hernia | |
| Wound infection |
Advantages of Mini Gastric Bypass (MGB) |
Disadvantages of Mini Gastric Bypass (MGB) |
|---|---|
|
|
|
|
|
|
|
|
|
|
|